End-Tidal Pepsi
In which a soft drink earns its place in the differential
There is a maxim in anaesthesia: no trace wrong place. The trace refers to capnography, which measures carbon dioxide in exhaled gas, and its output – a rhythmic waveform rising and falling with each breath – is our gold standard for verifying that an endotracheal tube sits where it should, in the trachea rather than the oesophagus.
The question arose in theatre, as these things do, in a quiet moment between cases. What if the patient had recently drunk something carbonated? The oesophagus connects directly to the stomach, and a stomach full of dissolved CO₂ is not entirely unlike a small, inefficient pair of lungs from the capnograph’s perspective.
Naturally, we felt obliged to find out. Sam, with admirable dedication to the scientific process, kindly donated a bottle of Pepsi to the cause.
The experimental setup was minimal. A spare reservoir bag, a CO₂ sampling line, and a willingness to look faintly ridiculous. We poured the Pepsi into the bag, positioned the sampling line above the opening to catch the escaping gas, and gently, rhythmically squeezed.
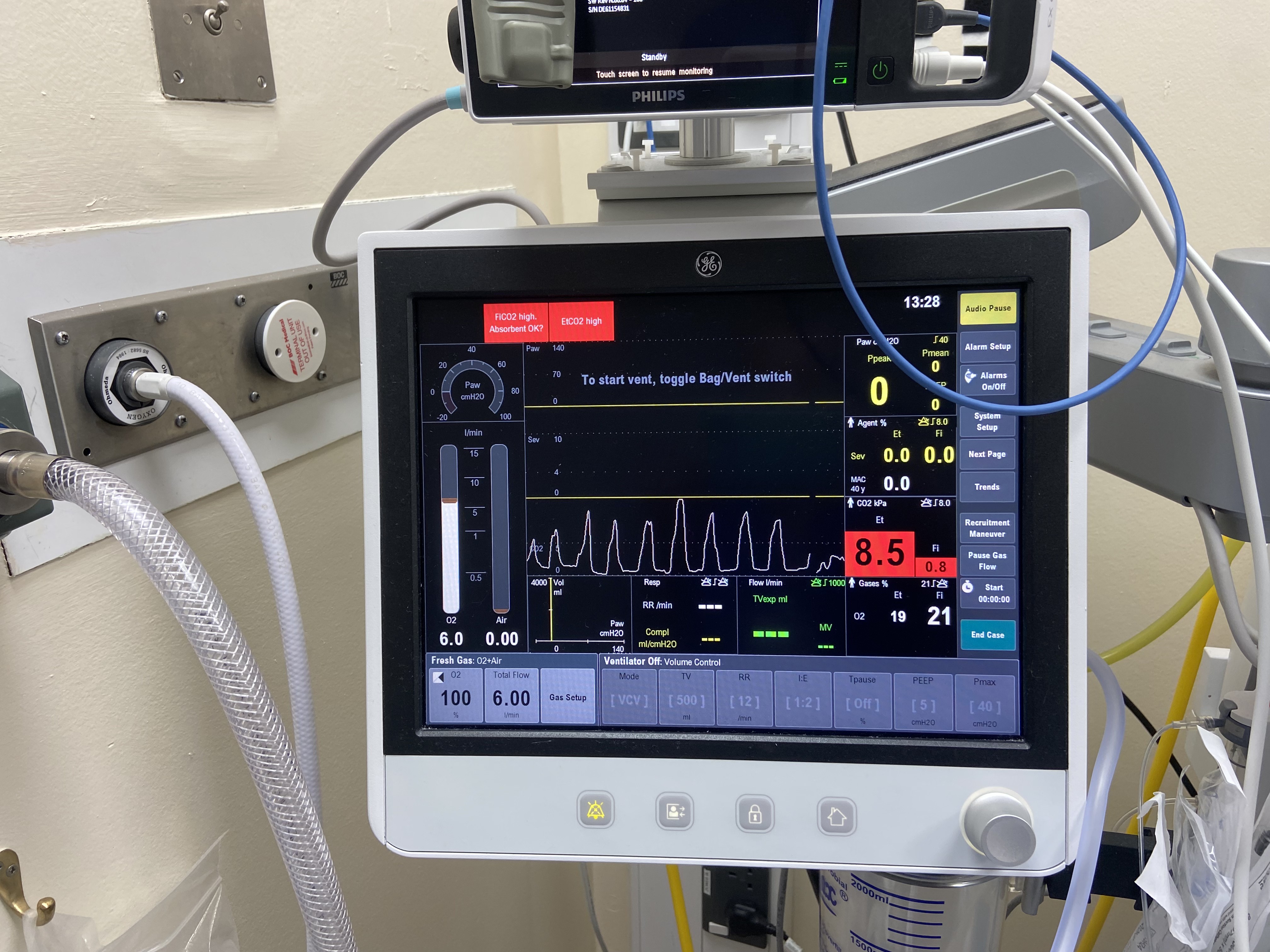
The trace was, as the photograph attests, entirely recognisable. Not perfect, the waveform lacks the clean plateau of a properly ventilated patient, but sufficiently convincing that a cursory glance at the monitor might not immediately raise alarm.
The practical upshot is not that capnography is unreliable. It remains the best tool we have, and the scenario requires a recently-carbonated patient, an oesophageal intubation, and inattention sustained long enough for the CO₂ to exhaust itself. What it does illustrate is that our monitors report what they measure, not necessarily what we assume they’re measuring. A waveform is not a diagnosis.
Sam deserves full credit for the experimental design, the procurement of consumables, and for not asking for the Pepsi back afterwards.